Taking Birth Back: Alums Give a Big Push For Midwifery

Jainee McCarroll ’93 with day-old Ellis, who was born with a midwife in attendance. “The support I had was all about getting Ellis here safely and in as simple a way as possible,” she says.
“My mother has very little memory of what it was like to give birth,” says Jainee McCarroll ’93. “She was knocked out and was traumatized by the experience. I wanted to shift the paradigm of my family’s birth history by giving my child the gift of my presence.” So when McCarroll went into labor with son Ellis in 2010, she did it awake and with a midwife’s help. “It was the most intense day of my life,” she recalls, “but the support I had was all about getting Ellis here safely and in as simple a way as possible. It felt like my greatest accomplishment, and I got to do it almost entirely on my own terms.”
For midwives, supporting a woman throughout her pregnancy and birth is equally powerful. Becca Van De Water ’00, a certified nurse-midwife practicing in Juneau, Alaska, says, “A midwife is there to be a best friend, sister, and healthcare provider all at once. My client is beloved to me by the time I’m catching her baby. I have a deep connection to her and all the people in her life. She’s not just a chart. She’s an experience.”
Midwife-attended births are an experience women throughout the world have had for centuries, and are still common in many countries today. In the United States, though, only about one in ten babies is delivered with a midwife’s help.
The numbers aren’t higher here due in part to lingering prejudice against midwifery and a relative lack of qualified midwives. A growing number of alumnae is active in combating the former and providing the latter.
Midwifery is still an often-misunderstood calling, they argue. And the fact that there are many different kinds of midwives, and that training and state licensing rules vary widely, doesn’t help. (Read about the different types of midwives at mana.org/definitions.html.)
The profession encompasses a broad range of services. Besides “catching” babies (a term midwives use in lieu of “delivering”), nurse-midwives, who account for the majority of midwives in the United States, provide services a gynecologist or nurse practitioner might provide, such as family planning, preconception care, pelvic and breast exams, menopausal management, and treatment for infections.
“The main difference between midwives and doctors, says Cynthia Lynch ’90, a certified nurse-midwife practicing in New York, “is that we don’t take care of anyone with a medical problem or whose pregnancy is not progressing within the normal range. We do everything an ob/gyn does, but don’t take care of people with diabetes,those who have heart problems, or those who need a cesarean (“C-section”). We deal with good, old-fashioned, normal pregnancy and birth.”

Midwife Becca Van De Water ’00 hands newborn Ruby to her mother, Ashleigh Ewing.
And midwives take their mission very seriously. Van De Water describes her entry into the profession as a spiritual calling. “It’s the deepest honor and blessing I’ve experienced in my life,” she explains.
“The first time I felt a fetus in the womb was a completely magical and transformative experience,” says Krystel Viehmann ’06, who is studying to become a directentry midwife. “When I placed my hands on that mama’s belly, I felt very strongly changed for the better.”
A Better Birth Experience?
Throughout history, midwives have served as a woman’s primary support during childbirth, but many women today are led to believe that modern medicine trumps the longheld knowledge of midwives.
“We tend to go along with what everyone else is doing, assuming it must be for the best,” writes Ina May Gaskin, founder of The Farm Midwifery Center in Tennessee, in Ina May’s Guide to Childbirth. “Living in a technological society, we tend to think the best of everything is the most expensive kind available. This is generally true, whether we are talking about cell phones, cameras, cars, or computers. When it comes to birth, it ain’t necessarily so.”
Elise Resch ’99, a certified nurse-midwife in a small, privately owned midwifery practice in Connecticut, notes that, “US maternal mortality and morbidity rates are perplexing. We spend more money and use more technology, but have worse outcomes.” For example, the World Bank’s most recent data show that the United States has a maternal mortality rate worse than virtually every European country, and many in Asia and the Middle East.
“American women are starting to ask important questions about why that is. They realize that one in three of them will have major abdominal surgery [i.e. a C-section] to have their babies—more than double the rate the World Health Organization (WHO) recommends. They are beginning to research their childbirth choices, including care providers, very carefully,” says Resch.
According to the American Pregnancy Association, C-sections can increase the risk of infection, hysterectomy, or injury to the bladder or bowel for mothers. Babies born by C-section are more likely to have breathing problems and difficulty breastfeeding. Additionally, more mothers die after C-sections than after vaginal births.
“Most births around the world lead to preventable traumas for mother and baby,” says Jan Tritten, editor of Midwifery Today. “Preventable because many of them are caused by unnecessary and scientifically unjustifiable interventions performed by hospital staff who do not understand how to properly facilitate the normal physiology of birth.”
One way of preventing these traumas, says the WHO, is by using midwives. Research suggests that, for healthy women likely to have low-risk births, midwifery births are safer, less costly, and more satisfying than typical medical-model childbirth. (Read more in the “Evidence-Based Maternity Care Report” at childbirthconnection.org.)
And given that more than 96 percent of births facilitated by certified nurse-midwives occur in hospitals, emergency care—should it become necessary—is nearly always close at hand. Resch, who delivers only at Yale New Haven Hospital, says women come to her because they think the skills and support of a midwife will optimize their chances of a vaginal birth and, hopefully, a meaningful experience.
“I felt it important not to medicalize [the birth process] so much,” recalls Jainee McCarroll. “When I needed medical attention, I was with a midwife who didn’t mess around. She took things seriously, but was also a calm, quiet force for simplicity. We’ve been conditioned to believe birth is a terrifying event, but your body knows what to do. Every cell of your body is summoned, and every cell answers the call.”
Protecting “Normal”
Why don’t more women choose this birth experience? For some, medical conditions make it inappropriate. But even midwifery’s supporters admit there is often a stigma attached to the profession. They trace it back to the early 1800s, when birth attendants in the United States began to shift from midwives to doctors. By the 1920s, home births, previously the norm, were relegated only to women without access to a hospital. This led to a pervasive idea that doctors were better suited to delivering babies, and midwives became marginalized and pushed out of public consciousness.
Slowly, however, a group of passionate women got the word out about the empowerment women could experience through actively choosing their birthing options. Around the 1970s, with the help of advocates such as Ina May Gaskin, midwifery was, you might say, reborn.
Still, America trails far behind other countries in using midwives. According to the National Center for Health Statistics, midwives attended only 7.5 percent of all US births. And a WHO report notes that the Americas average only one midwife for every 20,000 people, the lowest ratio of the six WHO regions worldwide.
One reason may be a perception that midwives lack training that would put them on a level comparable to doctors. Many people may not realize, says Suzanne Wertman ’90, a certified nurse-midwife in North Carolina, that most US midwives have at least a master’s degree from a major university. “I think women who aren’t our clients might think we’re uneducated, ‘crunchy granola’ types, and unsafe,” she explains, adding, “but the women who see midwives for their care are our best and most enthusiastic supporters.” Women such as Jainee McCarroll. “When I tell women about the level of care I received, they’re astonished,” she says. “Two days before I gave birth, my midwife came for a house call. You’d be hard pressed to find an ob/gyn who would do that.”
“We listen, we take the time to get to know our patients, and we trust a woman’s body,” says Wertman. “I wish everyone knew the benefits and how, with a change in focus from disease management to health promotion—using the midwifery model of care—we could have healthier moms and babies in the United States.”
To midwives, a “healthy” birth means a vaginal birth with as little medical and surgical intervention as possible. In some circumstances, medical intervention is crucial, but the midwifery community believes that, in doctor-administered deliveries, medicine and C-sections are often used when not medically necessary, and can largely be avoided.
“The medical model for childbirth is more about labor management than it is about honoring the body’s natural response process,” says Cynthia Lynch. “Doctors have a time frame and want people to be on the curve. If you fall off that curve, they give you drugs and medicalize your birth. They look at pregnancy as a disease process; midwives look at it as a normal function of the body,” Wertman agrees, “Medicine should only be used when needed, but we’ve gotten used to it as being normal. Let the baby come when it’s ready.”
“I have wonderful support from a team of high-risk obgyns who collaborate with us if our patients become highrisk or require a cesarean,” says Resch. “They are excellent specialists and surgeons when our patients need them, but the majority of the time, they don’t.”
Even in unusual circumstances, medical interventions aren’t always wise. For example, one frigid Alaskan winter, a client of Van De Water’s didn’t make it from her hotel to the birthing center in time. When Van De Water arrived at mom and baby’s side, “the baby was nursing, but the paramedics wanted to take them both through the cold air to the hospital for what was probably no good reason,” she recalls. “I stayed three hours to watch them, and they were fine. I think that gets at the heart of midwifery—being creative, solving problems, and protecting ‘normal’ from outside intervention.”

Suzanne Wertman ’90 (left) was midwife to Kerri when she gave birth to Scarlett (right). Wertman currently works for Planned Parenthood, but hopes to return to “catching babies” soon.
When all goes normally, the results are rewarding. Jen McGonagle Dziedzic ’01 gave birth to daughter Emelia at home, with her husband and a midwife by her side. “We had been trying to conceive for a while; then we had nine months of waiting,” she recalls. “To have my daughter at home made everything feel complete. There was so much joy—not throw-a-party kind of joy, but snuggle in bed, hang out with family, stare-at-her-and-be-amazed kind of joy.”
Stigma Remains
In addition to the long, unpredictable hours and the sometimes life-and-death nature of the work, midwives often must fight the medical establishment for recognition, respect, and pay.
“Midwives face a powerful medical lobby when it comes to trying to improve things on a state or national scale,” says Krystel Viehmann. “Out-of-hospital birth centers can now be reimbursed by Medicaid—the first necessary step toward getting midwifery services reimbursed by insurance and included in universal healthcare. We are professionally trained, legitimate healthcare providers. Being seen or treated as anything less has widespread ramifications for women’s choices as well as for the quality of their healthcare.”
“One of the big struggles is getting acknowledgement that we are incredibly trained healthcare providers who happen to practice in some ways that run along a different philosophy than that of the medical world,” echoes Van De Water.
“We struggle with medical insurance reimbursement rates that get smaller and smaller every year,” adds Wertman. “We worry about providing the kind of care women want in a system that rewards interventions and efficiency over relationships and outcomes.”
Malpractice fears, high insurance, low pay, and a perceived inequality within the medical field are realities midwives face, but that hasn’t deterred women (including at least twelve MHC alumnae) from entering the profession.
“Sometimes I get really exhausted from my job, but I keep going back because I know I am called to do this,” says Van De Water. “I’m there for the woman step-by-step through this life process. Midwifery is built on what has been done forever, but we have one foot firmly planted in the medical world. I’m grateful for science, but also for the other foot, which is placed firmly in tradition. I just trust that birth works.”
Resch couldn’t agree more. “The battles continue—to practice, to get covered, to get reimbursed, to break down misconceptions—but as we know, the will of women is strong, and they seem to be taking birth back.”
—By Stefanie Ellis
This article appeared in the fall 2011 issue of the Alumnae Quarterly.
MIDWIVES TAKING BIRTH BACK
For a primer on midwifery, a glossary of midwifery terms, and more, visit alumnae.mtholyoke.edu/midwives.
The International Experience: Dhanashri Patil ’13
Student Edge Extra: Extended Comments from Dhanashri Patil ’13
Dhanashri Patil ’13, who hails from Gondawale, India, talks more about her experiences as an international student at MHC
Coming to the U.S. and adjusting to everything (food, weather, culture, transport, the education system, etc.) was not an easy task for me but like everyone else, I have managed to do it and the first few months at Mount Holyoke seem very distant now.
Arrival
The visa process went smoothly for me as I received the documents I needed on time and the application was pretty straightforward. Even though I did not need tax help until later, I feel McCulloch Center did a great job at helping international students. They offered workshops and I got all the help I needed in filing my tax return.
Getting to South Hadley from Boston was a problem. There was only one ride from college that would bring new students on campus and I missed it. I had no idea how the bus system worked in this country and had to call the McCulloch Center’s office multiple times to know how I could get here.
I had a little trouble exchanging money after arriving on campus. I had cash in Indian rupees and when I contacted Bank of America they said that due to legal restrictions they could not exchange Indian rupees. So I had to send the cash to my friend in Boston who exchanged it for me at Logan Airport. This process took a long time and I wish there was something I could have done to get the money quickly.
Orientation
Even though at the time I felt like it was a long orientation, now I think it was necessary. It was a good time to get to know other students and get our questions answered by MHC students in an informal setting. Moreover, the college provided free calling cards to international students and I truly appreciated it. That was the only way I could call my parents and tell them that I had arrived safely. I was not in touch with them for almost four days after I left my country and they were really worried. Overall, the orientation team did a wonderful job. I do think they could add more practical things to the experience, such as treasure hunts on campus and making trips to the other five colleges and the Hampshire Mall on PVTA buses, so that we could get to know our way around. (I had hard time finding my way around this campus for almost three weeks!) Even though I had bus maps and schedules with me, I got lost a few times (May be it’s just me).
Friends
I mostly hang out with international students and do not really spend time with domestic students as much as I would like. I think this is the case with most international students here. I think it’s because international students go through similar situations with cultural shock, adjustment to food/weather, educational system etc., after arriving here and this leads to easier bonding.
I would say that culturally, things can sometimes be hard. For instance, initially I could not tell if a person I knew was my acquaintance, classmate or a really good friend. People here have different ideas and expectations about friendships than back home. For instance, I was told that just saying “hi” or talking about how a class was did not necessarily make someone your friend. Also, if someone is your friend, it does not mean they would want to go have lunch with you when you run into them. They can just tell you that they don’t feel like eating with anyone that day and that it has nothing to do with you. All this has taken some time for me to adjust to but now I am mostly correct when I interact with friends and other people.
In the classrooms, I do see international students (and sometimes myself) having trouble speaking up. It is mostly because they are not expected to speak up in the class in their home countries, and interrupting a class to ask questions is mostly considered as a rude gesture. In my case, when professors make it clear that we can ask questions or speak up, I am much more comfortable doing so.
The SAW Center is a great resource to work on writing if we need help. They are happy to read a paper just to see if there are any grammatical errors. One thing that I still cannot improve is use of the passive voice. It is perfectly okay to use the passive voice in papers in India in Hindi, English, and my mother tongue, Marathi. However, after coming here I was told that I should try to not use it. I am still trying.
Plagiarism
Plagiarism was a new issue for me while writing papers at Mount Holyoke because here it is taken much more seriously than what I am used to. In fact, I did not even know much about what counts as plagiarism and what doesn’t. I had to learn to be very careful while citing and quoting authors in my papers and introducing ideas. I appreciate the fact that my professors made me aware of this issue early on in my first semester. If some workshops were offered for new students on campus to inform them about “right writing” practices, it would be a great help.
Help Adjusting
But overall, I have seen that the professors are aware of the fact that international students have come from different academic backgrounds and they are willing to help us adjust to this environment. In some cases they are willing to go over our papers before we submit them to make sure that they re in the right format and correct writing style. In my first year I found this lenience to be of immense help and I think this aspect helps make Mount Holyoke a truly international educational institution.
—By Dhanashri Patil ’13
More Books: Fall 2011
Fairy Tale Capitalism: Fact and Fiction Behind Too Big To Fail
BY EMILY EISENLOHR
(AuthorHouse)
Financial analyst Emily Eisenlohr reveals the poorly understood financial products and deals leading up to the recent banking crisis. In simple terms, she explains over-the-counter derivatives, counterparty risk, credit ratings, and how risk-management practices and mergers tie the biggest banks together. Residential mortgage securitization is a major component of the disaster outlined in Too Big To Fail.
Emily Eisenlohr ’73 spent two years researching and writing this book, drawing on twenty years in the financial services industry, first as a Citibank corporate vice president and then as a senior credit officer at Moody’s Investors Services.
The Magic Door
BY MARINA JONES
(AuthorHouse)
A third-grade teacher, Marina Jones found that her students struggled to grasp the concept of measuring time. Rote memorization of math vocabulary didn’t help. So she wrote this story centered around Old Man Millennium, who stumbles on a magic door to the universe. Inside, time is easily visualized with cute illustrations, and repetition and simple language help young readers discover the patterns of time.
Marina Jones (MA’98) teaches at Coburn Elementary School in West Springfield, Massachusetts. This is her first book.

Web Extras for "30 Years of Red Ribbons"
HIV/AIDS-Related Links Suggested by Alumnae Interviewed for our Article
Tracie Gardner ’87
Recommended by Tracie Gardner
The Legal Action Center is the only non-profit law and policy organization in the United States whose sole mission is to fight discrimination against people with histories of addiction, HIV/AIDS, or criminal records, and to advocate for sound public policies in these areas.
LAC provides legal advice and representation to New York State residents who have HIV-related legal problems, especially due to discrimination or breach of HIV confidentiality or testing rights. They also help with problems such as health care proxies, living wills, permanency planning, and government benefits.
There is an FAQ section pertaining specifically to people with questions regarding HIV positive status and the work place.
The Body: The Web’s largest source of HIV and AIDS information.
The Body is a very comprehensive site, with everything from articles by medical experts and advocates including Tracie Gardner. They offer an “Ask the Experts” forum where site users can submit their questions. They also host dozens of bloggers who write about their own experiences living with HIV. The bloggers are an incredibly diverse group, and nearly anyone looking to find a common experience could connect with the stories of one of the bloggers. Additionally, the site includes sections on prevention, treatment, and living.
Young Women of Color HIV/AIDS Coalition
This organization aims to address increasing HIV rates among women of color aged 13–24 through building partnerships with individuals and organizations that serve and empower adolescents. The site provides access to information, allowing young women to make informed decisions; promotes personal and professional growth; and works to create a collaborative environment for youth-serving organizations.
The mission of AIDS United is to end the AIDS epidemic in the United States. They aim to achieve this goal through national, regional, and local policy/advocacy, strategic grantmaking, and organizational capacity building. With partners throughout the country, they work to ensure that people living with and affected by HIV/AIDS have access to the prevention and care services they need and deserve.
The site has a fact sheet for each state in the country which gives the breakdown on the number of cases in each state, county demographics, gender demographics, and so on.
AIDS Alliance for Children, Youth and Families
AIDS Alliance for Children, Youth and Families is a national nonprofit membership organization established in 1994 to give voice to the needs of women, children, youth, and families living with and affected by HIV and AIDS.
The Education and Training page lists numerous programs and conferences to assist care providers, women, and children affected by HIV/AIDS. These programs train participants to become advocates and mentors within communities. Included: The Consumer Leadership Corps Training Program, The Community Leadership Initiative Program, Girls 4 HOPE, VOICES.
The New York State AIDS Advisory Council
The New York State AIDS Advisory Council consists of 17 representatives from the public, educational, and medical communities, local health departments, and nonprofit organizations, including the advocacy and service community.
This site has a very clinical appearance, and features a myriad of resources and links to other resources, including youth outreach, healthcare for the uninsured, funding opportunities and statistics.
GMHC calls itself the world’s first and leading provider of HIV/AIDS prevention, care and advocacy.
This comprehensive site offers information on nearly everything, including how to get tested, how to lower one’s risk factor, and services for men, for women, and for children. GMHC also offers meals to individuals affected by HIV/AIDS, as well as access to mental health services.
Housing Works is committed to ending the twin crises of AIDS and homelessness.
Their mission is to provide people living with HIV/AIDS with access to quality housing, information on HIV prevention and healthcare. They were the first nonprofit in the country to use a self-sustaining model, meaning that the proceeds from their bookstore café, thrift stores, and catering company support the mission of the nonprofit.
Voices Of Community Activists & Leaders (VOCAL) is a statewide grassroots membership organization in New York building power among low-income people who are living with and affected by HIV/AIDS drug use and incarceration, along with the organizations that serve this population, to create healthy and just communities.
More about Tracie Gardner’s work
Watch a 15-minute presentation by Tracie Gardner on “The Politics of HIV Prevention: Black Women and the Fight for HIV/AIDS prevention Justice”
Synopsis: Gardner emphasizes the disproportionate number of black women with HIV relative to the whole population of women with HIV. She focuses on two age groups–young girls/teenagers and women over 45. She makes several suggestions which could relatively easily lower the occurrence of HIV:
1. Talk to women and girls about HIV. She says there is no point in pretending that young girls are not sexually active, and informing them about safer sex practices could dramatically lower their risk of infection.
2. Different branches of social services must communicate with one another. Women must have access to all manner of information, no matter what bureau or institution they go to for that information. There must be HIV/AIDS centers in places where women can get to them.
3. She says that men in the prison system are not receiving adequate care. Prisons must step up their healthcare provisions not only for the inmates, but for the population outside of the system (such as the families men return to after their prison sentences end).
Read Tracie’s article “Mandates Won’t Save Our Kids from HIV — Actual Follow-Through Will” at thebody.org.
Recommended by Mona Bernstein

Mona Bernstein ’74. Credit: Jude Mooney
AIDS.gov has links to federal resources and funding opportunities. There is also a section outlining the uses of new media to contribute, connect, and share information relating to HIV/AIDS.
Project Inform fights HIV and Hep C epidemics by helping individuals to make informed health decisions, advocating for affordable quality healthcare, and promoting medical strategies to prevent new infections. Their events calendar informs visitors when and where they can get involved in/attend fundraisers for the cause.
Technical assistance offered through the site is available to grantees and planning councils.
Kaiser Family Foundation offers all sorts of articles and fact sheets regarding HIV/AIDS, everything from Medicare/Medicaid, uninsured coverage, and women’s health, to minority health.
San Francisco AIDS Foundation offers information on risk, testing, and treatment. Client services include housing support and benefits counseling, as well links to support for minority groups who are at higher risk for infection with HIV/AIDS, including black men and Latinos.
The site has standard info from getting tested to prevention and treatment; has a questions and answer section, fact sheets, and brochures.

Aleefia Somji ’09 (right) and MHC friend model T-shirts intended to prompt conversations and shift attitudes about HIV.
Recommended by Aleefia Somji
Avert.org is “the most up to date all the time, and really great for general information about HIV,” says Somji.
The site is a comprehensive and user-friendly website with history of HIV/AIDS, testing prevention, quizzes, games, and stories. Has a section devoted to sex, sexuality, and relationships, and one devoted to HIV/AIDS around the world.
Elizabeth Pisani
The book The Wisdom of Whores: Bureaucrats, Brothels, and the Business of AIDS, by Elizabeth Pisani is “amazing, one of my favorites. The author is funny and really comes at the whole HIV issue from an epidemiological public health standpoint. Easy for anyone to understand. She’s done a lot with HIV,” says Somji.
Pisani also gave a 2010 TED talk “Sex, Drugs, and HIV—Let’s Get Rational” that provides a look into the logic used by addicts, which is an entirely different logic than is present in the mind of non-addicts. For example, Pisani and her team interviewed users in Indonesia asking them if they knew how HIV was spread. Nearly 100% said through the sharing of needles, yet 3 out of 4 users interviewed shared needles anyway, the reason being that if they were found on the street carrying a needle, they could be taken to jail.
Nawal El Saadawi
The book Woman at Point Zero by Nawal El Saadawi “is also great,” says Somji. “She’s an Egyptian author, its a true story.” The New York Times Book Review said of it, “Saadawi writes with directness and passion, transforming the systematic brutalization of peasants and of women into powerful allegory.”
This 2009 TED talk by Hans Rosling is described as having “new facts and stunning data visuals.”
“Helping Individual Prostitutes Survive: On the Van”
This article in The Body, is a three-part article that provides a firsthand glimpse of how a small-scale organization called HIPS (Helping Individual Prostitutes Survive) goes into the red light district of DC after hours and distributes what sex workers need to stay safe and stop the spread of HIV. Somji volunteers with this organization.
And the Band Played On (1987 book by Randy Shilts—and 1993 HBO film —about the early days of the AIDS epidemic). “It includes everything—health policy, the people who were tracking it, politics, economics, public health, quick decisions, its amazing. Highly recommended,” says Somji of the film.
More about Somji’s work
Read more about Aleefia Somji’s “HIV Positive” work while a student at MHC and in London.
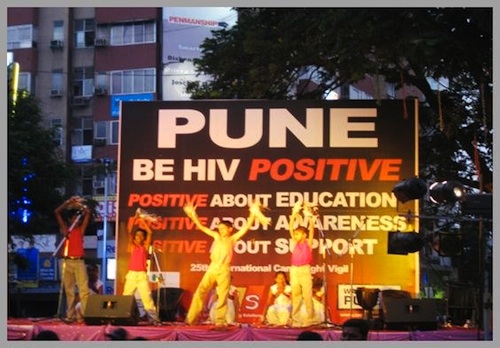
Wake Up Pune: “This is the website for the HIV Positive campaign and the first HIV organization I volunteered with, where I learned what disruptive theatre is, and where I met some of the most inspiring people ever,” says Somji.
Even More AIDS Resources:
Good magazine’s changing face of AIDS infographic brilliantly illustrates the successes and failures of the world’s fight against HIV/AIDS over the past three decades.
Alumnae Arden O’Connell ’97 and partner Liz Berges ’94 started Coalition for Courage after spending a year working and living in Zimbabwe at an center for HIV/AIDS orphans. The nonprofit now runs a scholarship program, and provides psychosocial support and food aid for the agency. They raise about $100,000 annually for the orphan-care center. Berges reported that one young woman they sponsored for six years has just finished her first year at MHC. She notes that there are two alumnae on the board and several others who work with the nonprofit on various projects.
More Alumnae Fighting HIV/AIDS
- Brooke Nichols ’09
Chelsea McCracken ’09 wrote the following about the work of her classmate, Brooke Nichols:
“Even as a young alum, Brooke has made an impact on HIV research and helped inform policy and funding decisions on both a small and large scale.
From her Mount Holyoke days through her master’s in epidemiology at UMass-Amherst, she spent a total of 6 months in Luderitz, Namibia, doing original research on the spread of HIV. She focused on alcohol consumption and migrant work patterns to better understand the epidemic. Her research concluded that having many informal drinking establishments in an area was linked to higher HIV prevalence, and after hearing her conclusions, the town put into place a program to register and formalize all of these drinking establishments. (She published a paper on her research in AIDS & Behavior: Nichols et al., “Density of Drinking Establishments and HIV Prevalence in a Migrant Town in Namibia,” 2011, in which she acknowledged Mount Holyoke for its financial support.)
She is currently working on her Ph.D. at the Erasmus Medical Center in the Netherlands, where she looks at the math modeling of the HIV epidemic in rural Africa. The first part of her Ph.D. has focused on seeing if “treatment as prevention” or “pre-exposure prophlyaxis” would be cost effective interventions. Because of this model, she was invited to the HIV Modeling Consortium, headed by Imperial College and funded by the Gates Foundation. She published a second paper, in the Journal of Internal Medicine, titled “HIV testing and antiretroviral treatment strategies for prevention of HIV infection: impact on antiretroviral drug resistance.” In October 2011, she also met with policy makers and mathematical modelers from around the world in South Africa to compare models and come to consensus on the similarities and differences among the models. This gave policy makers and major funders the opportunity to give their input on the models, discussing what would help them make funding decisions for different prevention measures.
She is now working on a mathematical model to investigate the potential emergence of drug resistance in Africa if treatment is scaled up. She is doing this in partnership with the World Health Organization, to help inform their policy decisions about antiretroviral therapy.”
- Elizabeth Berges ’94 and Arden O’Donnell ’97Coalition for Courage Helps Kids Affected by AIDS, PovertyBy Heather Baukney Hansen ’94
When I glanced at a toddler standing by the side of the road with a tiny pink Mount Holyoke College T-shirt on, I did a double-take. It was still morning but the strong African sun had already burned off most of the night chill. It was late last July and Elizabeth Berges (’94) and I were walking along a buzzing main street in Norton, Zimbabwe. We were nearly 8,000 miles from it, but here was this compact, powerful flash of South Hadley. I came to learn how closely linked the two—our alumnae and this stricken suburb of Harare—actually are.
It was my first time in Zimbabwe but Berges is a regular. She and Arden O’Donnell (’97) founded Coalition for Courage (C4C) eight years ago, to support vulnerable children in the region. Working with a local non-governmental organization, they sponsor scholars from pre-school through high school and beyond, financing school fees and uniforms, stocking a library, funding food security and teaching vocational skills.
By investing in these bright children with shy smiles and deep wells of desire in their eyes, C4C focuses on a groups that’s been lost amidst global revulsion at their nation’s tyrannical regime. During his 30-year reign, President Robert Mugabe has left widespread collateral damage in his wake. Several years ago, the economy virtually collapsed, taking with it the educational, health and agricultural systems that were once the envy of Zim’s neighbors.
Some staggering statistics represent the profound tears in its once-vibrant fabric: roughly 1.3 million, or one-fifth of all Zimbabwean kids, have lost at least one parent, most of whom died of AIDS. A solid quarter of the population is HIV-positive, and more than half of all new infections are among young people. Most of these are girls, largely because prostitution puts food on the table. This pandemic, compounded by political instability and poverty (more than half the population lives on less than $1 per day and the unemployment rate is somewhere between 70 and 80 percent) makes children, in particular, susceptible to exploitation and abuse. Zimbabwe gets the lowest donor support of any southern African nation for people living with HIV; $4 per person annually; compared to its neighbor Zambia, which receives $184 per person, per year.
But, while the global community stepped back, C4C and a remarkable number of MHC alums, stepped forward.
Berges and O’Donnell started C4C, in part, because when they returned from living there several years ago, they found that the hundreds of people who’d been getting their emailed dispatches from Norton were eager for updates on the kids. “I thought it strange at first because these people hadn’t even met them, hadn’t heard their laughter, hadn’t been there when their parents died,” says Berges. They hadn’t witnessed children sleeping on cold dirt floors sharing a blanket with siblings, crowding around one textbook with 20 others in class, or playing soccer in bare feet so they didn’t ruin the one pair of shoes they preserve for school. They hadn’t seen any of this firsthand, yet they cared.
For O’Donnell, founding C4C was also intensely personal. After her father died of AIDS in 1999, she got a Master’s degree in public health and requested a field placement at an orphan care center with kids who had lost their parents to HIV. “Losing my dad was so hard, I felt lost and alone,” she says. After spending six months in Norton, O’Donnell says, “I fell in love with the place.”
Alongside the tangible support, of school fees and the like, is a more abstract commodity that C4C gives kids: someone who believes in them. “They helped me realize my potential and significance in the world by their support and kindness,” says Jane Mugovi, who was a C4C scholar from sixth grade until she entered college. She is now a sophomore at Mount Holyoke. Mugovi lost both parents before she was 16 but, when searching for role models, she found confident, determined ‘MoHos,’ (as she calls us) all around her. In the essay that got her into MHC, she wrote, “In my view these women believe in the supreme worth of any individual … After learning they were all Mount Holyoke graduates, I knew that I wanted to be part of the community where they learned.”
The MHC/C4C circle is a wide one; some are generous donors with a deep connection maintained through letters, and others have been fortunate enough to have endured sporadic electricity, no running water and the biggest, creepiest spiders I’ve ever shuddered at, to meet some of Norton’s most clever kids.
Bethany Sager (’96) has sent the proceeds of her elementary school’s Hunger Awareness banquet to C4C for many years—a contribution which has grown from $700 to $7,000 in the past decade. She visited Norton in 2007 and was wonderstruck by the experience. “The children we worked with had such happiness in their hearts,” she says. One of Sager’s fifth-grade students was so inspired that, after raising money for two years, he hand-delivered soccer uniforms and balls to Norton.
Bridget McBride (’94) is a registered nurse, but it was a basic knowledge of sewing that helped her make a lasting impact during a two-week visit to Norton in 2010. She spearheaded the “Real Pads for Real Women” project and taught an entrepreneurial group of girls to make durable, reusable sanitary pads (disposable ones are prohibitively expensive there). The girls are now selling their product and reinvesting their profits. The Pads project is part of C4C’s on-going goal to help kids become sustainable adults with safe and healthy work through skills-building.
When asked why MHC women gravitate toward C4C’s work, she says, “Our time at MHC remains special in our hearts because it represents our first taste of the potential for powerful change both as individuals and a group,” and C4C is a chance to effect that change.
While they’ll admit to, at times, feeling frustrated and hopeless at the sheer scope of their undertaking (O’Donnell says working in Zimbabwe can be like “doing social work on the Titanic”) they can’t imagine quitting. “I deeply believe in the resiliency of children and…I am inspired by their will to succeed despite the circumstances of their lives,” says O’Donnell.
Like the MHC women before me, I think often about those little ones who flocked around this summer, under the intense African sun, to hear me read. They’d sit on my lap, hold my hand or sit just close enough to pinch my shirtsleeves. I smile thinking about the pre-schoolers who eagerly showed off their burgeoning English skills. “HowAreYouI’mFine! HowAreYouI’mFine!” they’d shout as Liz or I passed their playground several times a day. My heart is also heavy recalling their burdens, their memories of losing a parent or a sibling, or of sexual abuse suffered.
It’s hard to say why so many Mount Holyoke women are connected to Norton. It may be that we learned long ago on that dynamic campus that we’re not defined by what separates us—be it thousands of miles or oceans of opportunity—but instead by what unites us. A smile, a shoulder to cry on, an aspiration, a need to be acknowledged; these are the pieces of our shared humanity.
— Annotations by Laurel Rhame ’12

Web Extras for "Taking Birth Back"
The Kids Health site offers an introduction to midwifery. The site covers the history of midwifery, what midwives do, different kinds of midwifery training, how to decide if a midwife is right for you, and how to find a midwife.
For Midwives and Future Midwives
Midwives Alliance of North America: In 1982, the Midwives Alliance of North America (MANA) was established as a professional organization for all midwives, recognizing the diversity of educational backgrounds and practice styles within the profession. Its goal is to unify and strengthen the profession of midwifery, thereby improving the quality of health care for women, babies, and communities.
As a leader in midwifery, MANA has been at the forefront of developing midwifery credentialing and educational organizations. In particular, the North American Registry of Midwives oversees a competency-based certification process for midwives, granting the title of Certified Professional Midwife (CPM) to those passing rigorous written examinations and testing of clinical experience and skills.
The Mothers Naturally site has a search engine to help locate a midwife in your area of North America.
KidsHealth.Org provides this guide to the various kinds of midwives in North America.
________________________________________________________________________________________________________
Midwife Glossary
Doula – Trained to provide women emotional and physical support in labor, birth and the postpartum period. They do not perform clinical care or diagnose and treat medical conditions.
Certified Nurse Midwife (CNM) – Trained and licensed in both nursing and midwifery, and often work in conjunction with doctors. CNMs possess at least a bachelor’s degree and are certified by the American College of Nurse Midwives.
Certified Professional Midwife (CPM) – Trained in midwifery and meets practice standards of the North American Registry of Midwives. Practice mostly in homes and birthing centers, and have no hospital privileges. Not every state allows CPMs to practice.
Direct-Entry Midwife (DEM) – DEMs are not nurses. They are trained in midwifery through self-study, apprenticeship, midwifery school or a college/university program, and may or may not have certification. They usually practice in homes and non-hospital birthing centers. Not every state allows DEMs to practice.
Lay Midwife – Educated through self-study and apprenticeships, and aren’t certified or licensed.
Certified Midwife (CM) – Trained and certified in midwifery, but not a registered nurse. Possess at least a bachelor’s degree and are certified by the American College of Nurse Midwives. Not every state recognizes certification.
________________________________________________________________________________________________

The Book that Led to Midwifery’s “Rebirth”
Ina May’s Guide to Childbirth, by Ina May Gaskin. Publishers Weekly described it this way: “Founding member and former president of the Midwives Alliance of North America and author of Spiritual Midwifery, Gaskin offers encouragement and practical advice in her upbeat and informative book on natural childbirth.”
__________________________________________________________________________
MHC Connections Are Everywhere!

The birth support team for Jainee McCarroll ’93 included midwife Catherine Clark (left) and friend Cynthia Lynch ’90. Clark’s mother is Lynn Butcher Clark ’56.
When Jainee McCarroll ’93 gave birth to son Ellis, her midwife (left) was Catherine Clark. McCarroll was surprised to learn that Clark’s mother was an MHC alumna too–Lynn Butcher Clark ’56. And McCarroll’s dear friend Cynthia Lynch ’90 (right) was her labor support from the beginning.
Suggestions from Jainee McCarroll ’93
- Ina May’s Guide to Childbirth (Most important book I read)
- Real Food For Mother and Baby (Second most important book I read)
- Hypnobirthing (Third most important book I read)
- The Birth Partner (Most important book—and only book—my husband read)
- Here is my midwife Catherine Clark’s Web site.
- Here is my postpartum doula Erica Shane’s Web site.